
A 15-year-old female presents with mild dyspnea with exertion, and frequent wet cough and throat-clearing. Her respiratory history is notable for asthma as a child, and 2 episodes of pneumonia and 2 episodes of influenza within the past year. A chest radiograph had shown a right middle lobe density during her second episode of pneumonia. She does not have a history of prematurity or chronic sinopulmonary infections, or symptoms of gastroesophageal reflux. She does not smoke tobacco products or use electronic cigarettes. There was no significant travel history and no pets.
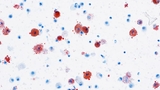
On physical exam, vital signs are normal. She has forced expiratory wheezes in both upper lobes, and no digital clubbing. A chest radiograph demonstrates mildly increased interstitial markings. Spirometry is normal, without significant bronchodilator response. Despite starting inhaled fluticasone (Flovent), a course of prednisone, and a 14-day course of amoxicillin-clavulanate to treat presumed protracted bacterial bronchitis, she has no improvement in symptoms and her dyspnea progressively worsens. High resolution computed tomography (HRCT) of the chest is performed. Expiratory views show patchy areas of air trapping bilaterally. She undergoes flexible bronchoscopy with bronchoalveolar lavage. (See Figure 1).
The answer to last issue’s quiz is burnout, the topic of this issue’s lead story. Congratulations to C.B. Melini, MD, of Marlton, New Jersey, who was the first of many readers to submit the correct answer.
A 15-year-old female presents with mild dyspnea with exertion, and frequent wet cough and throat-clearing. Her respiratory history is notable for asthma as a child, and 2 episodes of pneumonia and 2 episodes of influenza within the past year. A chest radiograph had shown a right middle lobe density during her second episode of pneumonia. She does not have a history of prematurity or chronic sinopulmonary infections, or symptoms of gastroesophageal reflux. She does not smoke tobacco products or use electronic cigarettes. There was no significant travel history and no pets.
On physical exam, vital signs are normal. She has forced expiratory wheezes in both upper lobes, and no digital clubbing. A chest radiograph demonstrates mildly increased interstitial markings. Spirometry is normal, without significant bronchodilator response. Despite starting inhaled fluticasone (Flovent), a course of prednisone, and a 14-day course of amoxicillin-clavulanate to treat presumed protracted bacterial bronchitis, she has no improvement in symptoms and her dyspnea progressively worsens. High resolution computed tomography (HRCT) of the chest is performed. Expiratory views show patchy areas of air trapping bilaterally. She undergoes flexible bronchoscopy with bronchoalveolar lavage. (See Figure 1).
The answer to last issue’s quiz is burnout, the topic of this issue’s lead story. Congratulations to C.B. Melini, MD, of Marlton, New Jersey, who was the first of many readers to submit the correct answer.