What is HLHS?Andrea Thrush : We got pregnant with Morgan in September of 2001.
Shane Thrush : We were married three years, and we thought now's the time, we're going to take the next step, and —
Andrea Thrush : Along she came.
Shane Thrush : We got pregnant relatively easily.
Andrea Thrush : Normal, happy pregnancy, planning —
Shane Thrush : You wonder the sex. You go through the names and making the room up, and —
Andrea Thrush : And then it take to that January morning.
Shane Thrush : As we were going through that January appointment, they were checking everything. Everything is fine. Everything is fine. We're all excited. We're joking around with the ultrasound tech. And then she stops talking. And that's when —
Andrea Thrush : That's when we had found out that she had a congenital heart defect.
Shane Thrush : Hypoplastic left heart syndrome.
Andrea Thrush : She was diagnosed at week 23.
Thomas L. Spray, MD : All of heart surgery is 50 years old, and we've come from a situation of being able to treat nothing to being able to at least deal with most, if not the vast majority of, congenital heart defects in a way that allows children to grow into adulthood.
Jack Rychik, MD : We live in an era where there are very few things that we really can't take care of.
Thomas L. Spray, MD : Even 20 years ago, we could not treat hypoplastic left heart syndrome successfully. Now it's become almost routine in most centers.
Sarah Tabbutt, MD : One of the things we're most well known for is moving forward the field for babies with hypoplastic left heart syndrome.
Thomas L. Spray, MD : And as things continually improve, and as these children have issues when they get older, I have no doubt we will have ways to treat those issues. So I don't see any reason to be pessimistic about the long-term outlook for these children.
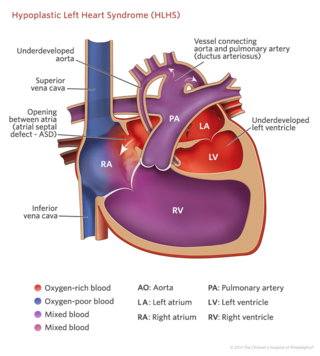
Jack Rychik, MD : Hypoplastic left heart syndrome, or HLHS, is a collection of diseases, collection of anomalies of the heart in which the left side of the heart, for whatever reason, is inadequate to do the job it's supposed to do in delivering blood flow to the body.
J. William Gaynor, MD : And it's grouped in a group of defects called single ventricle, where there's really only one pumping chamber to the heart.
Jack Rychik, MD : In order to understand and to comprehend any of the different forms of heart disease that exist, it's very important to make sure we understand what the healthy or the normal heart looks like. The normal heart has two sides, a right side and a left side, and four chambers, the top receiving chambers, or atrium, and the lower chambers, which are thick-walled pumping chambers called ventricles. Red blood cell will come from either the superior vena cava or the inferior vena cava and enter into the right atrium. The blood then flows across the tricuspid valve to the right ventricle. The right ventricle then squeezes and ejects that blood cell into a vessel called the pulmonary artery. The pulmonary artery splits into two vessels, each going to the lungs. As that red blood cell makes its way through the lung, it returns through the pulmonary veins to the left atrium. That blood is now oxygenated. It's picked up oxygen, then goes across the mitral valve into the left ventricle, which does most of the work in terms of delivery of blood flow to the body. That blood cell is now ejected into the aorta to some organ or muscle or skin in the human body. Now, there are some significant differences between the heart in the newborn and the heart in the fetus.
Elizabeth Goldmuntz, MD : The heart actually is — assumes its almost complete anatomy often before a woman would even know she was pregnant.
J. William Gaynor, MD : The heart is actually functioning and pumping blood to the baby throughout most of fetal life.
Jack Rychik, MD : Because the lungs are collapsed in the fetus and it's really the placenta through which much of the oxygenation takes place through the mother, there are various bypass pathways within the fetal heart that direct blood away from the lung. The first is a structure called the foramen ovale. That's communication between the two top chambers of the heart that allows for blood to go from the right atrium to the left atrium. In fact, because there is very little blood that's returning from the lung which would normally go to the left side, the majority of blood that fills the left atrium and left ventricle is coming across the foramen ovale from the right side. Because the lungs are collapsed, there's high pressure, high resistance in the lungs. As blood is ejected out the right ventricle and enters into the main pulmonary artery, very little goes down into the lungs themselves. The majority goes into a structure called the ductus arteriosus, which is the second important communication between the pulmonary artery and the descending aorta. The third structure that's important that connects the umbilical vein to the fetal circulation is a site, a junction, called the ductus venosus. That acts as somewhat of a resister, if you will, in terms of controlling the return of blood from the placenta to the fetal circulation. Birth is a wonderful process and an amazing process, and there's a dramatic change that takes place in what we call the fetal transition, this transition of the circulation from fetal life to neonatal life. As soon as the cord is clamped, the ductus venosus ceases to carry blood to the heart, and it begins to constrict within the first few hours or days of life. The very first thing that happens when a fetus is born is it takes its first breath, the lungs expand, and so the resistance or pressure in the lungs drop, and that promotes blood flow into the lung itself. The ductus arteriosus begins to constrict and is typically fully closed within 24 to 48 hours of life, and blood is now then fully directed into the lung. As the blood returns to the left side of the heart, after traversing the pulmonary circulation and picking up oxygen, the pressure in the left atrium rises just a bit, and the trap door of the foramen ovale, which was open before birth, now begins to close, usually within the first few days of life. So one can imagine that if you are solely dependent on your right ventricle to do the job of delivering blood to the body, once that ductus arteriosus begins to constrict or close, then there's no way for blood to get to the body, and unfortunately these babies — these babies die.
Peter J. Gruber, MD : But if we know a complex lesion is coming up, a child that's suffering from one of these, we can prepare for that ahead of time.
J. William Gaynor, MD : We can avoid having a sudden cardiac arrest at home, or even death, sudden death at home, by knowing that the baby has the heart defect. If necessary, we can arrange to have the baby delivered at CHOP —
Thomas L. Spray, MD : In a much more controlled treatment strategy. So that's a huge advantage in terms of prenatal diagnosis.
How HLHS DevelopsJ. William Gaynor, MD : Hypoplastic left heart syndrome, which some people call HLHS, is one of the more common forms of congenital heart detects.
Peggy McCann, RDCS : There's a couple things that make up the HLHS variant, and the number one is usually small left ventricle and associated with all small left-sided structures. By that, I mean a small mitral valve, a small aortic valve, a small left ventricle, and a small aortic arch.
J. William Gaynor, MD : There's almost infinite variety in the actual clinical findings.
Peggy McCann, RDCS : And typically, during the initial scan, things will be apparent on the ultrasound right away.
Zhiyun Tian, MD : So each piece of the information are very important. We actually can help the physician provide information to the family.
Thomas L. Spray, MD : Basically, hypoplastic left heart syndrome is a situation where there is an underdeveloped left ventricle.
Peter J. Gruber, MD : That's usually the pumping chamber that pumps blood from the heart to the rest of the body.
Thomas L. Spray, MD : It can involve the mitral valve, which is the valve entering the left ventricle; it can involve the left ventricle itself; and it can involve the aorta, which is the artery leaving the left side of the heart to the body.
J. William Gaynor, MD : The aorta, which carries blood to the body, is frequently very small and blocked.
Thomas L. Spray, MD : The ultimate problem here is that the left ventricle cannot support the circulation.
Peter J. Gruber, MD : So without a left side that's big enough, it's not strong enough to provide blood flow to the body.
J. William Gaynor, MD : It's a very severe form of heart disease, and if not treated medically — and then surgically — early after birth, almost every infant will die within the first few weeks of life.
After DeliveryThomas L. Spray, MD : What we want to do after a baby is born is we want to stabilize the child, make sure that there are no other organs involved, because there are other associated anomalies in some children. We want to make sure that there are no genetic issues that we need to address. We want to make sure all the other organ systems are as good as they can be and assess them if we have to. And then once that is done, then it's more a matter of scheduling the surgery.
J. William Gaynor, MD : For many children with complex heart disease, there's blockage of the blood, either going to the body or to the lungs. And there's a blood vessel called the ductus arteriosus which connects those two arteries. Everybody has one, and it usually closes after birth.
Sarah Tabbutt, MD : You can keep that blood vessel open with a medication called prostaglandins. And so, therefore, by giving a baby prostaglandins, you're actually replicating the same physiology that it had in the uterus, when it was very stable, to when it's outside the uterus.
J. William Gaynor, MD : So instead of having a child come in critically ill, where there was nothing we could do, we can stabilize these children, do diagnostic procedures, and then have a stable child who goes for surgery.
Thomas L. Spray, MD : If you just leave a child with this circulation for a period of time, then they end up going into heart failure because so much blood goes to the lungs in a circle that they end up in heart failure. So you have to walk a balance between the two. You have to have the ductus open and eventually control how much blood goes to the lungs. That's why the operation is done usually in the first week of life.
Jack Rychik, MD : Through our experience with hypoplastic left heart syndrome in the fetus, we've been able to identify a variety of factors which function as risk factors for outcome for these patients.
J. William Gaynor, MD : One of the things that can cause a real problem is when there's blockage to blood flow from the lungs getting back to the heart.
Thomas L. Spray, MD : There are rare children who have what's called an intact atrial septum, and these children are the most difficult to deal with with hypoplastic left heart syndrome.
J. William Gaynor, MD : In hypoplastic left heart syndrome, the blood that comes back from the lungs comes to the left side of the heart. But because there's only one pumping chamber, it has to cross over to the right side of the heart inside the heart to be able to pump out. That's normally done through a hole in the wall between the two upper chambers of the heart called a foramen ovale. Some children we see where there's a very tiny hole and the hole is restrictive. Sometimes we can see where there is no hole, and the atrial septum is completely closed.
Thomas L. Spray, MD : This complete closure of the partition between the upper chambers of the heart means that blood that gets back to the left side of the heart can't go anywhere.
Jack Rychik, MD : That results in an increased back-up pressure on the pulmonary veins.
Thomas L. Spray, MD : So right after birth, we have to do something very quickly to open up that partition.
Jack Rychik, MD : And the way that's done is by passing a catheter across the atrial septum, blowing a small balloon up —
Jonathan J. Rome, MD : And you pull it back very quickly, and you literally rip a hole between the two upper chambers. That allows the blue and the red blood to mix now, and then they get — the children become much pinker. They have oxygen in their bloodstream, and they're stabilized so that they can basically survive until they can have surgery.
Thomas L. Spray, MD : And that can allow the resistance in the lungs to drop enough to consider the Stage I operation, usually after five or six days.
Jack Rychik, MD : Oftentimes, even when these babies are born and we immediately open the atrial septum, there can already be difficulties with the way the lungs have formed. And that can add a risk to these patients. We know also from our experience that if there are any extra cardiac abnormalities besides the heart disease itself, that can add risk to the reconstruction of the heart in HLHS. And we also know that if there's a known genetic abnormality, that can add risk. And then finally, there's the issue of prematurity. Although we're now able to care for babies with HLHS very, very well that are very small, if there is significant prematurity and immaturity, or lack of normal development of the lungs and other organ systems, that can add significant risk to the overall operation.
Robert E. Shaddy, MD : So if an amniocentesis test hasn't been done or a chorionic villus sampling test hasn't been done prior to the patient being referred, then we can help to coordinate that, either with the referring doctor, or we can take primary responsibility for getting that testing done here.
RepairJack Rychik, MD : Our current strategy for reconstruction of the heart for HLHS involves three stages, one done initially at birth, one at approximately three to six months of age, and the third stage at approximately two to three years of age.
Thomas L. Spray, MD : This is not an operation that creates a normal heart.
Jack Rychik, MD : We can't fix the heart.
J. William Gaynor, MD : We cannot make another pumping chamber.
Thomas L. Spray, MD : What we do surgically is rearrange things, close holes, make connections —
J. William Gaynor, MD : So that you can have blood going to the lungs and blood going to the body with only one pumping chamber.
Thomas L. Spray, MD : But that isn't the same as a normal heart.
Jack Rychik, MD : By rerouting the plumbing, we normalize the circulation.
J. William Gaynor, MD : And that procedure that does that is called the Fontan operation.
Thomas L. Spray, MD : The principle of the Fontan operation was really that if you had low resistance in the lungs, that is, if blood could pass through the lungs without much difficulty, then you didn't have to have a pumping chamber pushing blood through the lungs.
J. William Gaynor, MD : However, you can't do it in a newborn. The lungs are too immature; the babies are too small.
Peter J. Gruber, MD : Essentially, the pressure in the lungs is too high —
Thomas L. Spray, MD : To allow blood flow to go through without something pushing it. So we already knew how to do a final operation for hypoplastic left heart syndrome. The problem was the first operation.
Peter J. Gruber, MD : We found a way to reconstruct this very difficult subset of patients who had single ventricle, those with hypoplastic left heart syndrome.
J. William Gaynor, MD : And that's called either the Norwood procedure or Stage I reconstruction.
Thomas L. Spray, MD : We like to do that surgery in the first week after birth, but it can be a day, two days, three days. It just depends on how stable the baby is. And the principles of that operation are to connect everything so that the one good pumping chamber, which, in hypoplastic left heart syndrome, is the right ventricle, that ventricle has to pump to the body. So you have to connect the arteries to the lungs and the body in such a way that all the blood goes out to the body without any obstruction.
Peter J. Gruber, MD : In HLHS, the aorta is usually too small. So we correct that by putting a patch on to enlarge it.
J. William Gaynor, MD : And that's done by connecting the pulmonary artery, which comes from the right ventricle, to the aorta and then usually putting a patch on to finish the connection of those two blood vessels and enlarge the aorta.
Thomas L. Spray, MD : In addition, you have to prevent blood from backing up inside the left side of the heart, so you have to cut out the partition between the two upper chambers of the heart. And then the third principle of the Norwood operation, or the first-stage operation, is to provide some restricted blood flow to the lungs.
Peter J. Gruber, MD : What we call pulmonary blood flow. And we do that by placing a shunt, or a small tube, from one of the systemic arteries, or arteries that goes from the heart to the body, to the pulmonary artery.
Thomas L. Spray, MD : That is enough flow that you can get enough oxygen in the blood stream but not so much flow that you have resistance problems because that resistance is what prevents you from doing any further surgery.
Susan C. Nicolson, MD : It's very, very important that the family feels comfortable with you, as an individual, taking their child from them, and that the child recognizes that nothing bad is going to happen to them, that they can do this without being awake for any painful experience.
J. William Gaynor, MD : They'll go to the operating room. The anesthesiologist will put them to sleep. We'll then clean, prepare everything in their chest and abdomen sterilely so that we can do the operation without infection. It's performed through an incision in the front, over the breast bone. And we put them on the heart-lung machine and cool them down to take care of their brain and other organs while we do the repair.
Peter J. Gruber, MD : We're bypassing the heart and the lungs so that the operative field, the area where we're working, is clean and we can see what's going on. The heart's generally not beating, although occasionally it is, but at least it's decompressed. There isn't blood flowing through it.
J. William Gaynor, MD : We'll then do the operation, warm them up, bring them off the heart-lung machine. We'll make sure that the heart is working OK, that the blood pressure is OK, that there's enough oxygen in the blood, that there's no bleeding. And then usually we leave a couple little tubes inside the heart to let us measure pressures in the heart and give drugs. These come out through the skin. There's also usually two little, blue pacing wires which let us change the heart rhythm. We then leave a drainage tube, and once everything is stable, the baby will come back up to the Intensive Care Unit, and the operation usually takes about three and a half to four hours.
Robert E. Shaddy, MD : We anticipate the hospital stay after surgery for hypoplastic left heart syndrome to be approximately two weeks. It can be longer, sometimes three or four weeks or even longer, if there are significant complications.
Andrea Thrush : She pulled through that with flying colors. She was in and out of the hospital in a week after her surgery. Her second surgery was when she was three and a half months old.
J. William Gaynor, MD : Once a baby has had the Norwood procedure, then eventually we're going to go to the Fontan operation. And in the Fontan operation, what we do is we connect the blood flow coming back from the body directly to the lungs. You can do it in one operation, but we've learned that babies do much better if we split it up and do it in two operations.
Thomas L. Spray, MD : When you have this single ventricle malformation, all the blood that goes to the lungs comes back to the heart, goes out to the body, and a portion to the lungs again. And the amount that is going to the lungs is an extra amount of blood that the heart has to pump. The second-stage operation, done somewhere between three and six months of age, generally, takes away that extra volume that the heart has to pump. And it does that by getting rid of the shunt, or getting rid of the blood flow to the lungs directly from the heart, and connecting the veins from the upper part of the body directly to the arteries to the lungs.
Peter J. Gruber, MD : You have to wait until the lungs essentially mature enough that you can provide a different source of pulmonary blood flow.
Thomas L. Spray, MD : This is called either a Bi-directional Glenn shunt or a Hemi-Fontan operation, half of the Fontan operation.
J. William Gaynor, MD : We go back through the same incision, and this is sort of the risky part of a redo operation because there's scarring from the first operation. And so we have to be very careful when we go through the breast bone that we don't damage the heart, the lungs, the aorta. And every now and then, there can be bleeding from the heart just because of the scar tissue, and we have to go on the heart-lung machine through other blood vessels, either in the neck or in the groin. It's rare to need to do that, but we're always ready to do that if we have to.
Thomas L. Spray, MD : Once we get to that second operation, the heart is in a much better condition, and usually the risk of that surgery is extremely low. And the risk after that surgery becomes quite low also, of any sudden event. So I always breathe a sigh of relief when we get to that second operation or that second-stage procedure because it's a much better physiologic situation for the heart.
Andrea Thrush : She did well with that procedure, as well. She was in and out of the hospital in five days. It was a little easier in that you know what to expect of the routine of the hospital, the staff that you're working with.
Thomas L. Spray, MD : The third-stage operation is a variant of the Fontan operation.
Peter J. Gruber, MD : And that generally takes place somewhere after two years, but the child's physiology really tells us the best time to do that.
Andrea Thrush : Her third surgery was when she was almost three and a half years old.
Shane Thrush : This last one was definitely tougher. She was well aware of what was going on, what was coming to her, and she still talks about it today.
Andrea Thrush : So it was hard for us leading up to that third surgery.
J. William Gaynor, MD : There are two types of Fontan operations. One is called the Lateral Tunnel Fontan, in which a baffle is placed inside the heart to redirect the blood flow from the lower part of the body to the lungs. The other is called the Extra Cardiac Fontan, where we actually use a tube that brings the blood outside the heart, up to the pulmonary arteries.
Thomas L. Spray, MD : But the Fontan operation is based on connecting the veins from the body directly to the arteries to the lungs.
Peter J. Gruber, MD : Normally, the inferior vena cava, which drains the bottom of the body, attaches to the heart at the inferior or bottom portion. And what we do is to literally divide this from the heart. We sew up the portion of the heart where the inferior vena cava entered, and then we sew a tube end-to-end to the remnants of the inferior vena cava. We take this tube and loop it around the side of the heart and sew it into a hole we make into the pulmonary artery. So we essentially bypass the entire heart.
Thomas L. Spray, MD : It's a more efficient connection because the tube is a very specific size, and the blood going through there is not turbulent. Turbulence loses power, and power loss is a problem if you don't have anything pushing blood through the lungs. It cannot work unless there's low resistance in the lungs. And the key is you have to have a good pumping chamber on the other side which essentially sort of sucks blood through the lungs.
Peter J. Gruber, MD : Now, the one modification is that we put a small hole in the side of the heart and in the side of this graft and sew it together with what's called a fenestration.
Thomas L. Spray, MD : And the reason we do that is that it's been shown that having that little hole, while it does allow some blue blood to mix with the red blood, it also decreases the risk of developing fluid around the lungs after surgery, something called a plural effusion. Effusions used to be the biggest problem after the Fontan operation. Children would have the surgery and do quite well, but they would develop a lot of fluid that collected around the lung, and they'd often have to have a tube in the chest for weeks or even months to drain that fluid. Nowadays, with the use of this fenestration, that is a very uncommon event, whereas it used to be routine.
OutcomesShane Thrush : At this point we're at an every-six-months appointment just for basic checkup and —
Andrea Thrush : It's the standard EKG, vital signs, oxygen levels, relatively brief checkups. They spend more time talking to each other and catching up.
J. William Gaynor, MD : Most babies with hypoplastic left heart syndrome born before the 1980s had no chance of survival.
Thomas L. Spray, MD : And many children are now in their early teens with this kind of heart condition, and they're doing quite well.
J. William Gaynor, MD : They're basically on a medical frontier. They're on the cutting edge of medicine right now.
Thomas L. Spray, MD : The surgery for hypoplastic left heart syndrome has evolved since the early 1980s and continues to evolve.
J. William Gaynor, MD : So really, a child who survived all this in the late ྌs is very different from a child having surgery today. So we have a moving target because we're getting better at what we do.
Thomas L. Spray, MD : Only time will tell what the long-term outcome really is.
Andrea Thrush : She is so full of energy. I mean, you can't even believe she has a heart defect. And people that don't know what she's been through look at her in awe of what she's capable of.
Robert E. Shaddy, MD : From a heart standpoint, most of these children are very good at adapting to their limitations. And so if they're on the playground, playing with other children, they will play with them and get around with them and limit themselves as they need to. In addition, we're finding out that there are also neurologic abnormalities that many of these children have and will have as they grow older, some of them with learning difficulties, some of them with ADHD issues, and some of them even more complex than this.
Sarah Tabbutt, MD : We've really pushed the field in, you know, making this a heart disease that is not only not fatal but is actually very survivable with good outcomes. And shouldered on that is the transition to trying to optimize neurodevelopmental outcomes, particularly for babies with hypoplastic left heart syndrome. And a lot of that information has come from this program.
Peter J. Gruber, MD : A number of these kids are grown up now and are doing well — they visit — having relatively normal lives.
Thomas L. Spray, MD : In terms of intramural sports, in terms of, you know, being able to do what other kids do in general, most of these children have done quite well and keep up with their peers. Many of these children will have issues when they get older. Some will require additional surgery. Some will require additional procedures of various types. Some may have rhythm problems that need to be addressed. And some will probably eventually need a heart transplant. But what I tell families is that there are more adults now than there are children living with congenital heart disease which, frankly, is a testimony to the fact we've been pretty successful at dealing with these conditions.
Robert E. Shaddy, MD : Our mission ultimately is to help children with heart disease and to help their families get through this difficult problem, to do whatever we can to make their lives better.
Andrea Thrush : When you, again, go from being told a diagnosis like hypoplastic left heart and feeling a lot of uncertainty and anxiety, you visit here, and you realize there's knowledge and compassion and comfort at CHOP.
Shane Thrush : You walk in here, and you just feel, you know, that Morgan's best interest is in their best hands, so —
Andrea Thrush : That's one of the reasons why we chose her middle name to be Hope, because it was such a strong feeling and sense that we got every time we came and left.
Elizabeth Goldmuntz, MD : What moves me is to work with the families and to work with the children and to give them the best possible care that we can provide. That's first and foremost.
Susan C. Nicolson, MD : And to see them grow and to see them integrated into the family and to see them interface with their parents and their siblings just as you would any other routine and normal child.
Thomas L. Spray, MD : To be able to take the heart of a child and fix it so that the physiology is better and the child has a chance at a long life, that's very gratifying.
J. William Gaynor, MD : There's nothing better than seeing the kids come back when they're four or five years old.
Susan C. Nicolson, MD :And really see that they're just like any other kid.
J. William Gaynor, MD : A child who had had hypoplastic left heart syndrome who — I walked in the Intensive Care Unit one day, he was six years old, and he was there with a broken leg. I said, "What are you doing here?" Well, he was out mountain boarding with his cousins. I'm really sorry he broke his leg, but I'm really happy that here's a child who 20 years ago would have been dead, and he's alive to be out mountain boarding with his cousins. That's why to do it.
Jack Rychik, MD : Through the Fetal Heart Program, we're now able to offer hope and promise for the future for these children to go on to lead happy and healthy lives. And that's what this is all about.